Real-World Evidence on Malaria Risk Factors in Children Under Five — Burkina Faso (IeDA 2017–2020).
Real-World Evidence Summary
Study Type: Retrospective longitudinal observational study
RWD source: IeDA electronic consultation data from primary health centers (CSPS)
Population: Children 2–60 months in IeDA districts (Burkina Faso, 2017, 2018, 2020)
Outcome: Clinical malaria episode at consultation (yes/no)
Method: Generalized Estimating Equations (GEE, logit link, exchangeable correlation)
Objective: Quantify the real-world association between demographic, nutritional, immunization, and infection-related factors and malaria risk under routine care conditions
Key insight: Age, HIV status, distance to facility, prior malaria episodes and seasonality strongly shape malaria risk; vaccination and malnutrition show age-dependent effects.
Overview
Real-world data (RWD) from electronic decision-support systems can capture disease burden and risk factors under everyday programmatic conditions that randomized trials cannot represent.
This study leveraged the IeDA platform — a digital clinical tool used in Burkina Faso’s primary-care system — to generate real-world evidence (RWE) on malaria risk factors among children under five.
The analysis reframes academic results into an RWE-compliant framework aligned with ISPOR/EMA real-world study design principles.
Real-World Data & Study Design
| Aspect | Description |
|---|---|
| Data Source | IeDA electronic consultations (CSPS facilities) |
| Geographic Scope | Multiple districts implementing IeDA |
| Study Period | 2017, 2018, 2020 (2019 excluded) |
| Study Population | Children aged 2–60 months with ≥ 1 consultation |
| Design | Retrospective longitudinal cohort (repeated visits per child) |
| Unit of Analysis | Consultation record |
| Perspective | Population-averaged effects at patient-encounter level |
Endpoint
- Primary outcome: presence of a confirmed malaria episode at each consultation
- Covariates: age (+ age²), sex, malnutrition status, HIV status, vaccination completeness (BCG, pentavalent, pneumococcal, polio, rotavirus), prior malaria episode, month of visit (seasonality), distance to facility, district.
Analytical Framework
The analysis used Generalized Estimating Equations (GEE) to model repeated malaria outcomes per child.
RWE Methodology Highlights
RWD Quality Controls: duplicate removal, harmonized identifiers, imputation of missing facility data, age-window validation.
Confounding Mitigation: multivariable adjustment; sensitivity cohorts (4–60 mo and 6–60 mo)
Effect Modification: age interactions tested for sex, nutrition, HIV, and vaccines.
Outcome Reporting: adjusted odds ratios (aORs) with 95 % CIs; p < 0.05 as significance threshold.
Insights
| Domain | Real-World Finding | Interpretation |
|---|---|---|
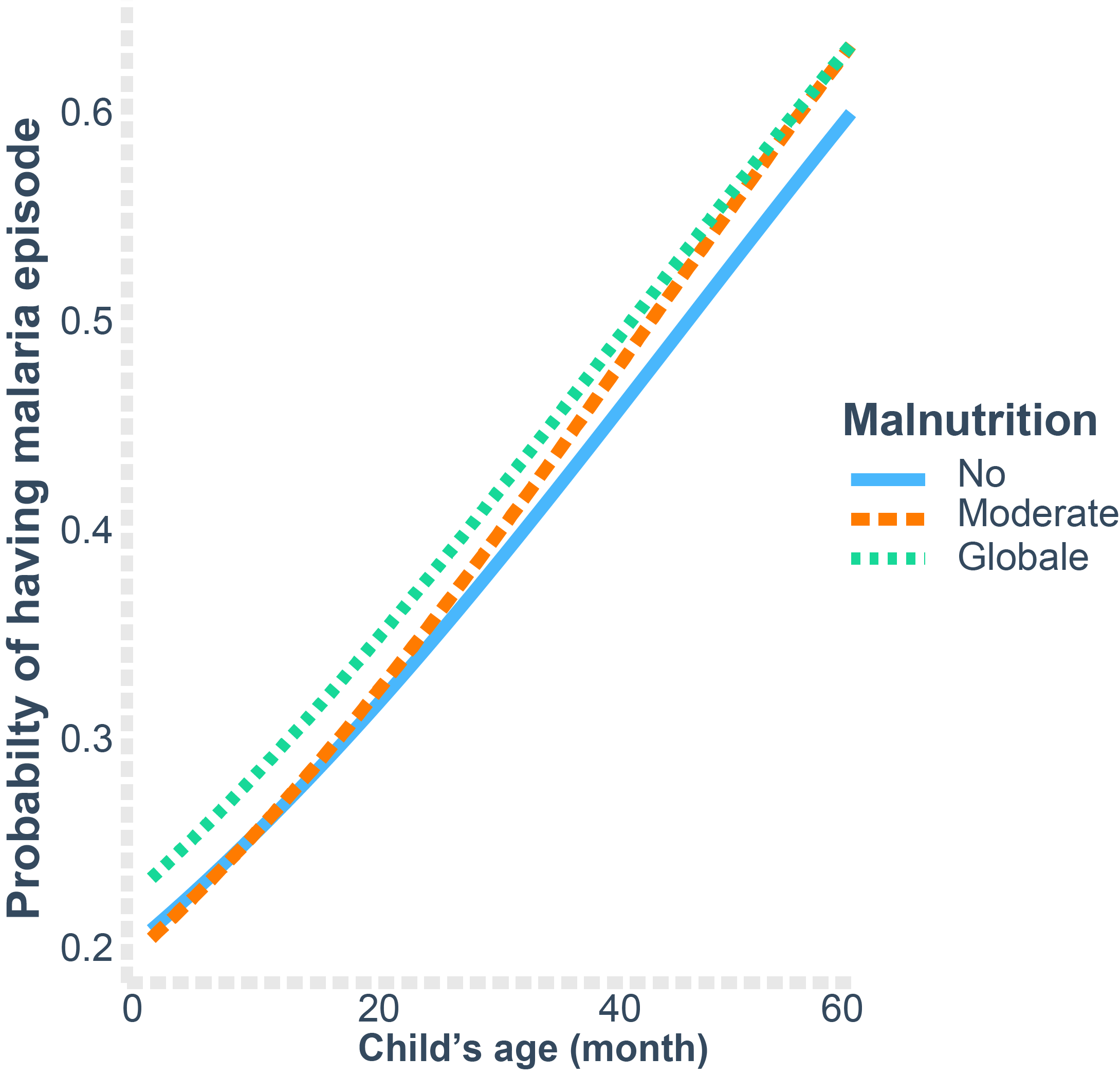
| Age | Malaria risk rises non-linearly with age (2 → 60 mo). | Likely reflects increased exposure and partial immunity. |
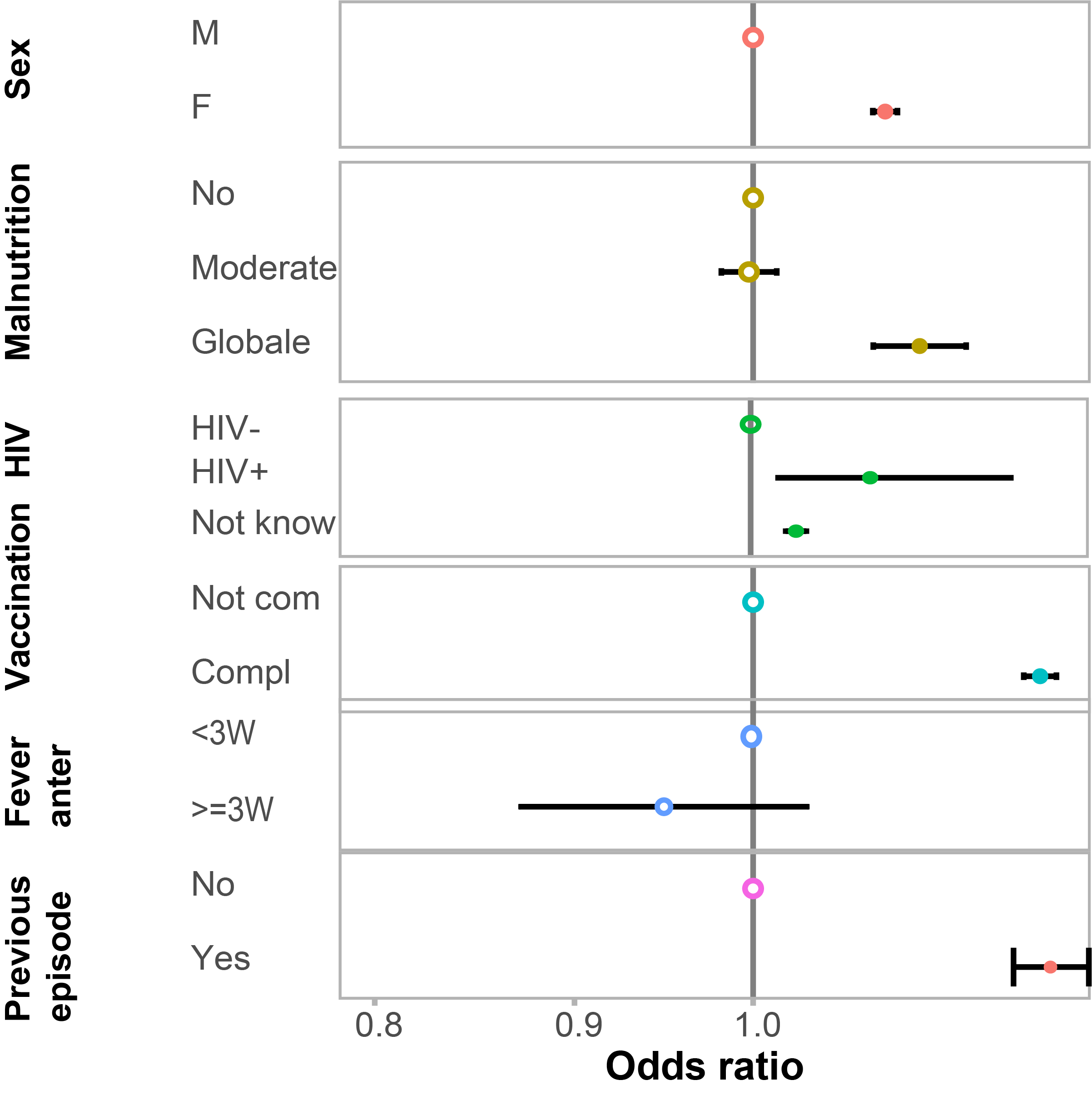
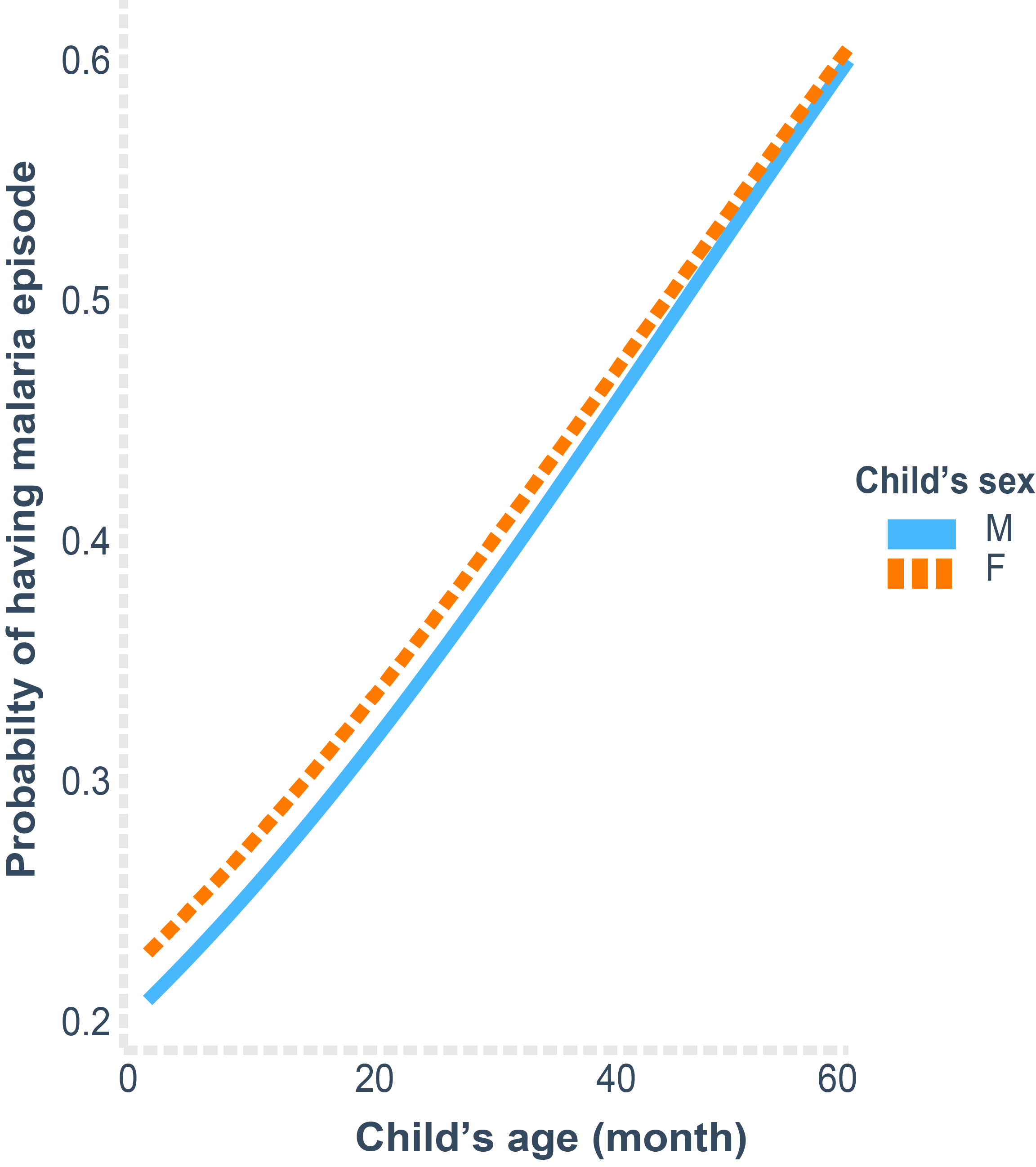
| Sex | Girls show slightly higher odds of malaria than boys. | Possible behavioural and biological differences. |
| Nutrition | Moderate/global malnutrition linked with lower observed odds. | May reflect health-seeking or survivor bias in RWD. |
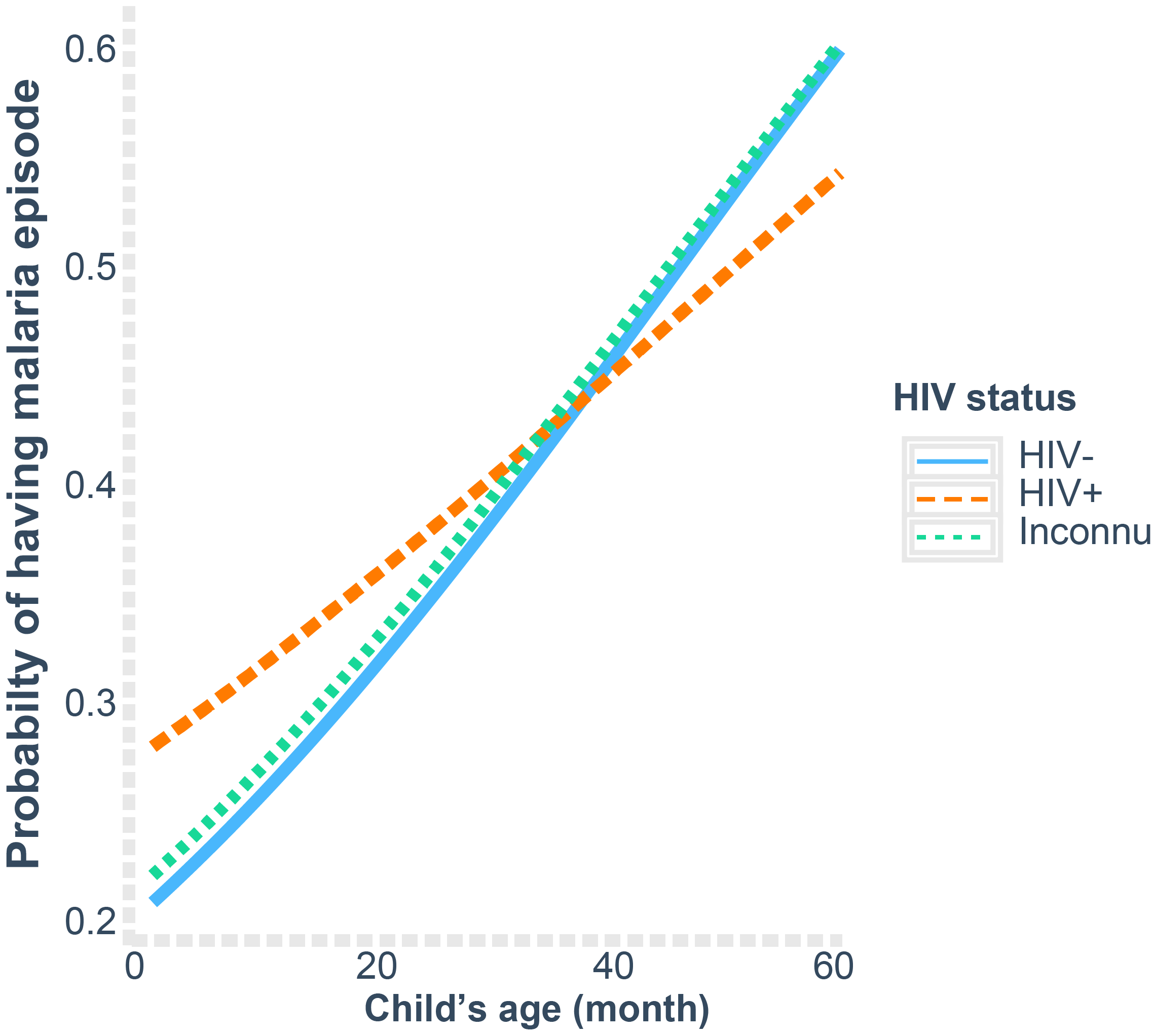
| HIV Status | HIV-positive children have 1.7–2.0× higher adjusted odds. | Aligns with prior longitudinal evidence. |
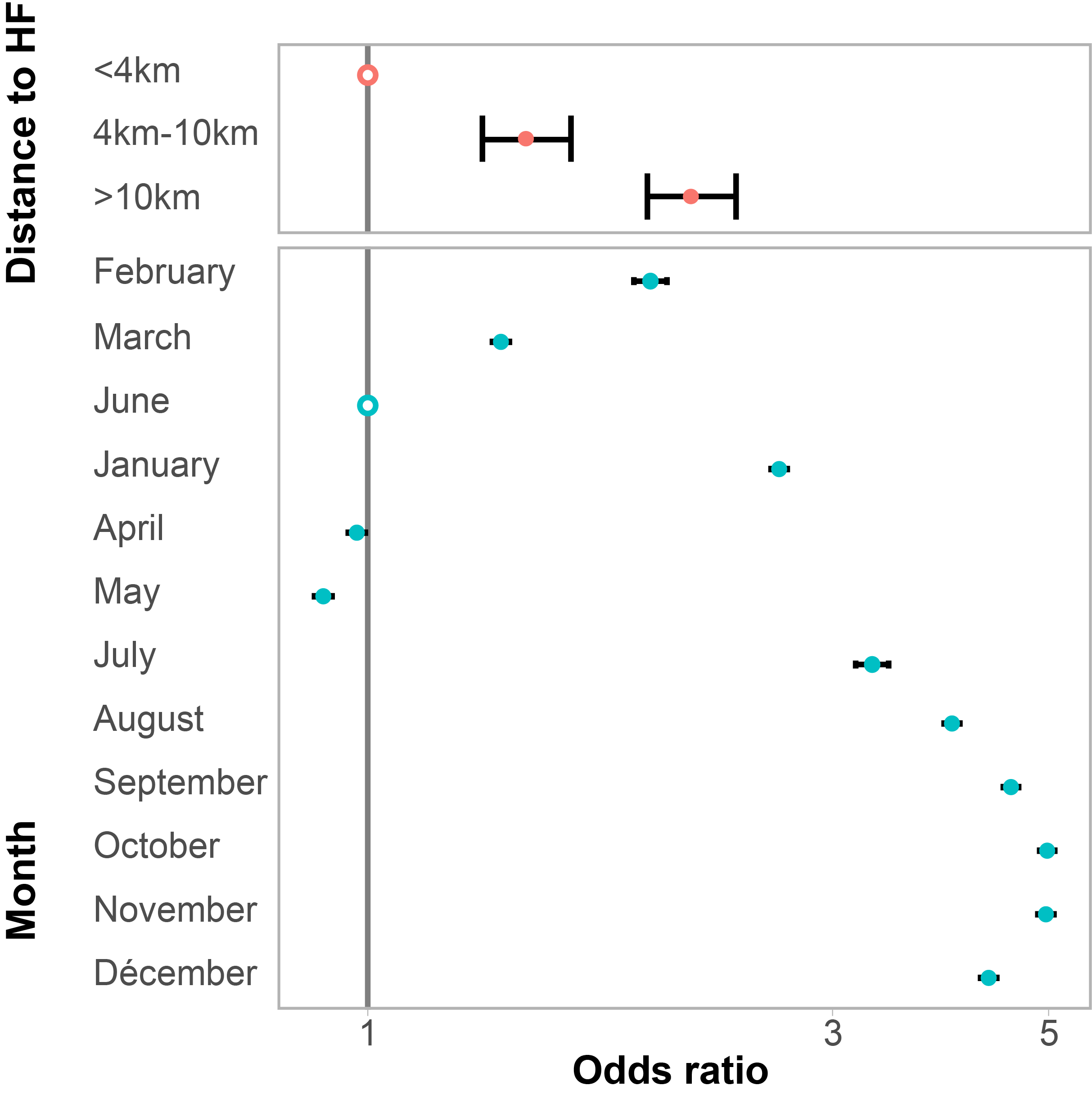
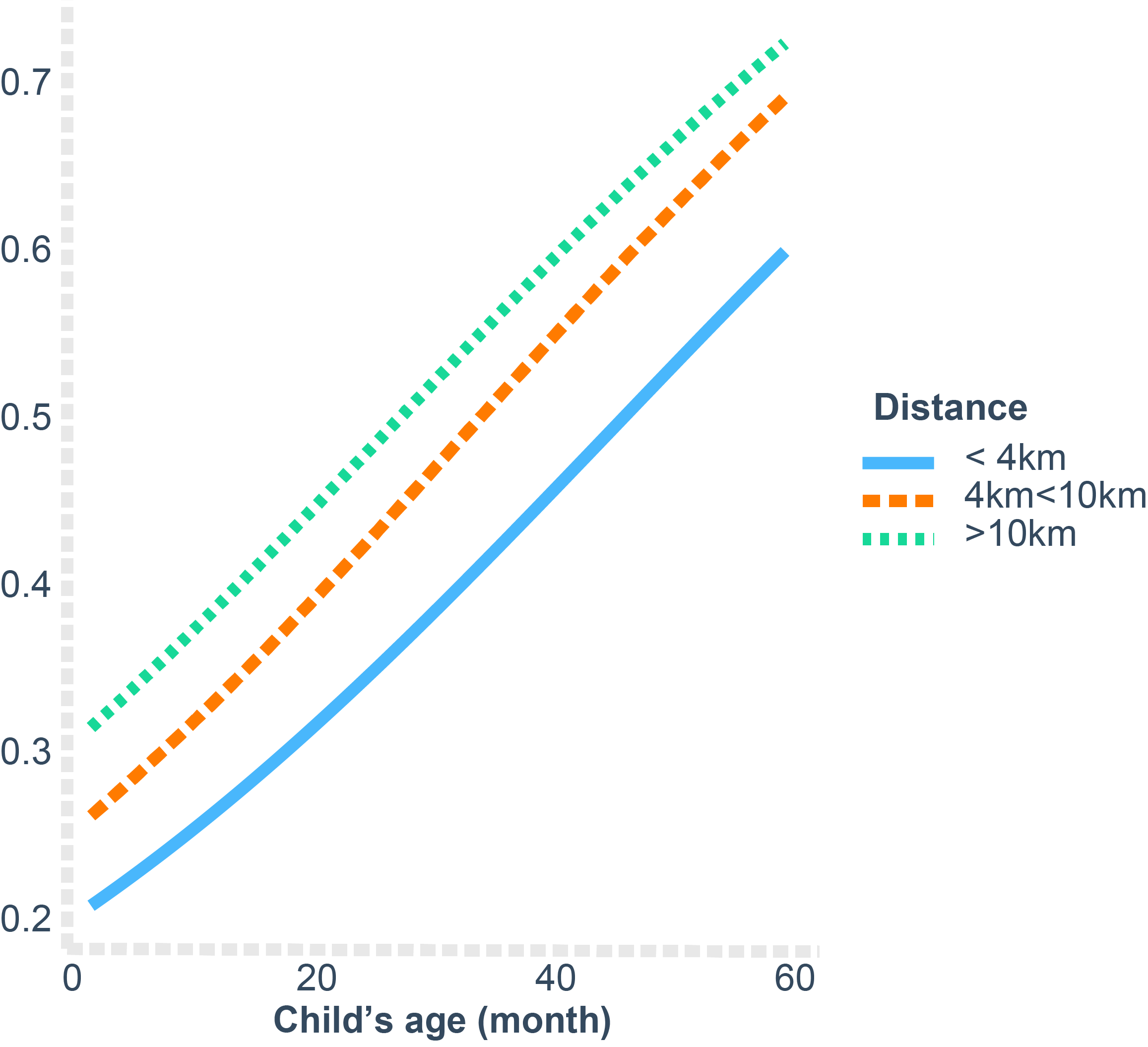
| Distance to Facility | Risk increases with travel distance (> 10 km > 4–10 km > < 4 km). | Indicates access barriers in real-world settings. |
| Seasonality | From July–October, malaria probability ≈ 3× higher than in May. | Confirms expected transmission peaks. |
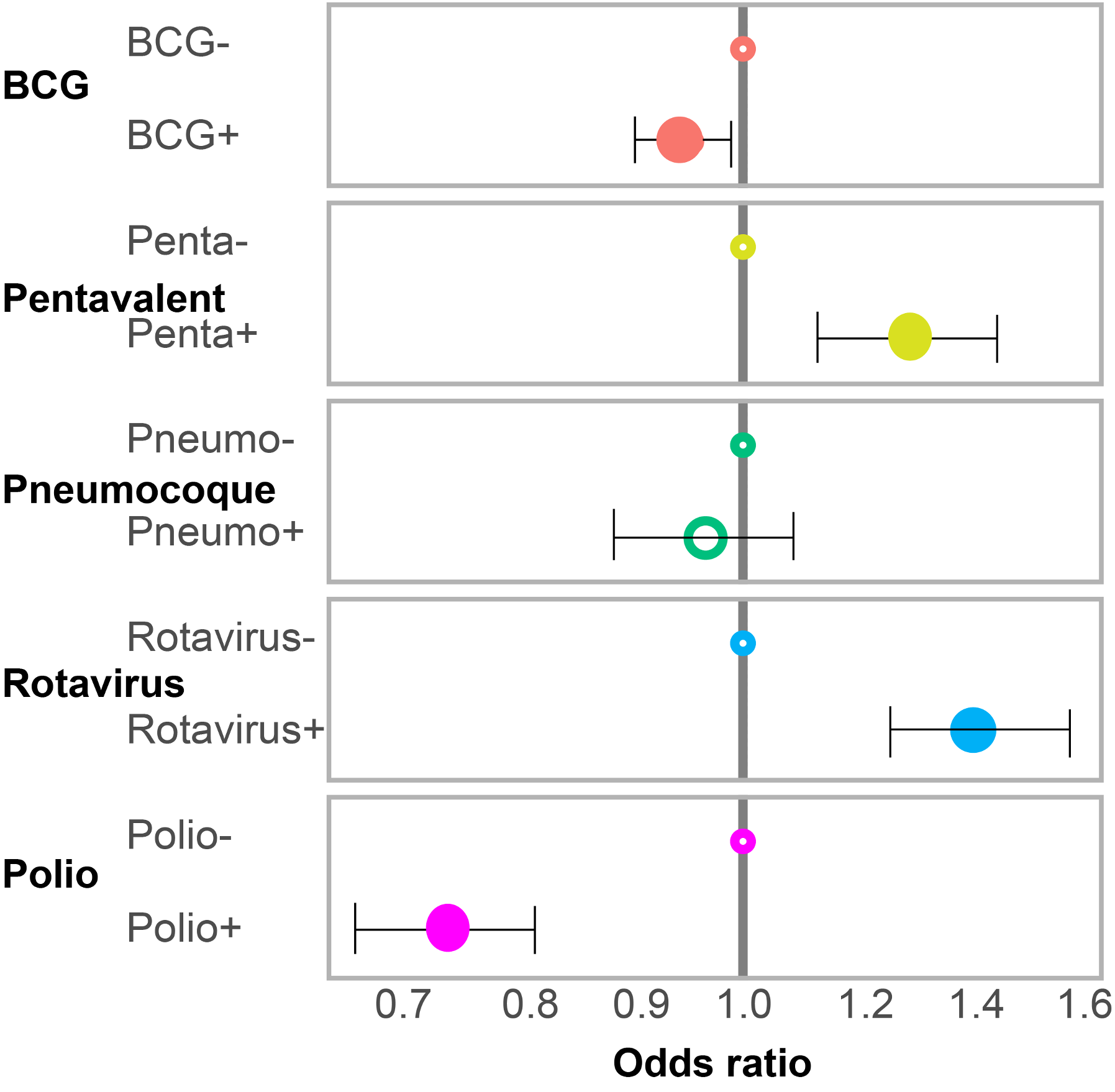
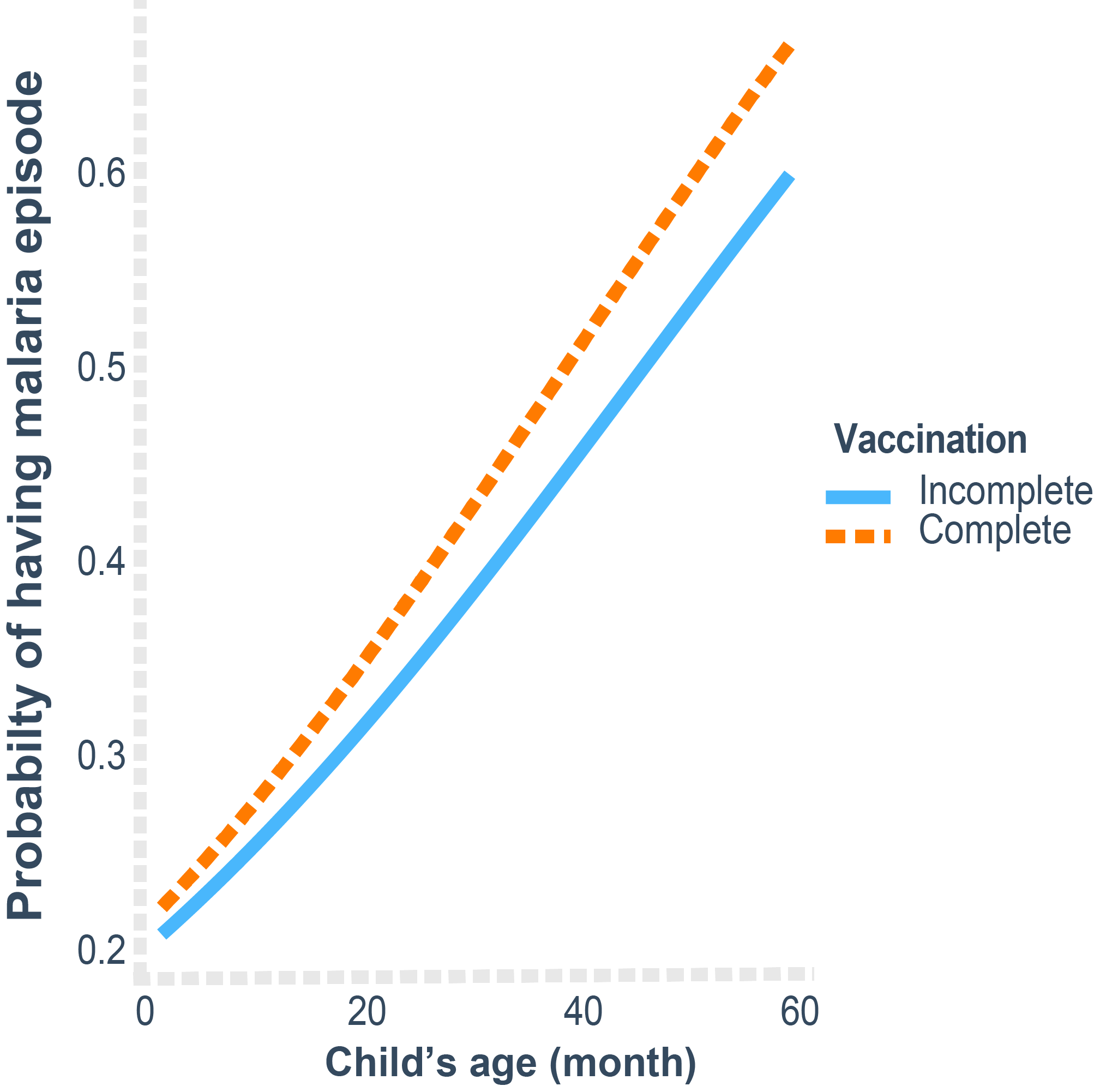
| Vaccination | BCG and other vaccines show protective trends but non-significant in adjusted model. | Reflects indirect benefits and data heterogeneity. |
Forest plots (single multivariable GEE model)
All three forest plots below are derived from the same multivariable GEE model (population-averaged effects with an exchangeable correlation structure).
For visualization purposes, covariates are grouped into three panels:
- Demographic and clinical factors (age, sex, prior malaria, HIV, malnutrition)
- Access and seasonality factors (distance to facility, month of visit, district)
- Vaccination status (BCG, pentavalent, pneumococcal, rotavirus, polio)
Age-modified effects (interaction plots)
To reflect effect modification by age, we extended the main GEE model with interaction terms between age and selected risk factors (e.g. sex, malnutrition, HIV status, distance, and vaccination).
The plots below show predicted probabilities of a malaria episode across age for key subgroups, based on the fitted interaction model:
- Age × sex
- Age × malnutrition status
- Age × distance to nearest health facility
- Age × HIV status
- Age × BCG / pentavalent / pneumococcal / polio / rotavirus vaccination
RWE Interpretation and Impact
Clinical relevance: The study demonstrates how longitudinal RWD can uncover real-world risk gradients across demographic and programmatic factors in pediatric malaria.
Programmatic insight: Results support integrated malaria–nutrition–immunization strategies and highlight access inequities (distance to facility, HIV coinfection).
Methodological contribution: Establishes a reproducible RWE pipeline using routine digital health data, showing that IeDA can serve as a valid RWD source for health-system performance and disease-risk monitoring.
Technical Skills Demonstrated
Real-World Data Management: large-scale data cleaning, QC, and cohort curation.
Statistical Programming: longitudinal modelling with geepack, broom, gtsummary.
Epidemiological Methods: GEE for correlated binary outcomes; effect-modification assessment.
RWE Reporting: alignment with ISPOR/EMA/ICH E3 guidelines; real-world endpoint definition.
Reproducibility: fully scripted Quarto workflow and transparent code base. :::
Ousmane Diallo, MPH-PhD – Biostatistician, Data Scientist & Epidemiologist based in Chicago, Illinois, USA. Specializing in SAS programming, CDISC standards, and real-world evidence for clinical research.
Back to top